Cubital tunnel syndrome: how you’re unknowingly damaging your nerves
Key points
Disclaimer
This information is for educational purposes only and is not intended to replace the advice of your doctor. Esports Healthcare disclaims any liability for the decisions you make based on this information.
The information contained on this website does not establish, nor does it imply, doctor-patient relationship. Esports Healthcare does not offer this information for diagnostic purposes. A diagnosis must not be assumed based on the information provided.
What is cubital tunnel syndrome?
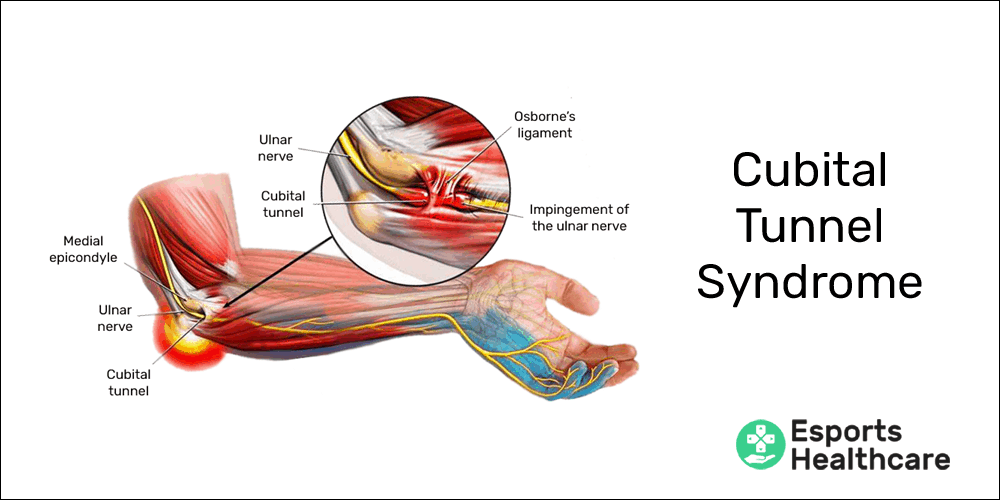
Cubital tunnel syndrome is an impingement or irritation of the ulnar nerve within the cubital tunnel at the elbow. This is the area commonly referred to as the funny bone. If the ulnar nerve becomes irritated in this region due to pressure, inflammation, and/or stretching, symptoms will occur.
Cubital tunnel syndrome is more prevalent in console gamers due to the position of the hands and arms while gripping a controller. If you’re a console gamer, you’re more likely to develop cubital tunnel syndrome if you lean your elbows on your knees or on the armrests of your chair.
Note: although more common in console gamers, PC gamers are not completely excluded from experiencing cubital tunnel syndrome. If you’re a PC gamer, you may still be at risk for developing cubital tunnel syndrome.
Pertinent anatomy
It’s important to know some basic anatomy of the elbow to understand cubital tunnel syndrome.
To begin, the word “cubital” in cubital tunnel syndrome is in reference to your elbow. The cubital tunnel is an anatomical passageway around the back of your elbow comprised of bones and fascia.
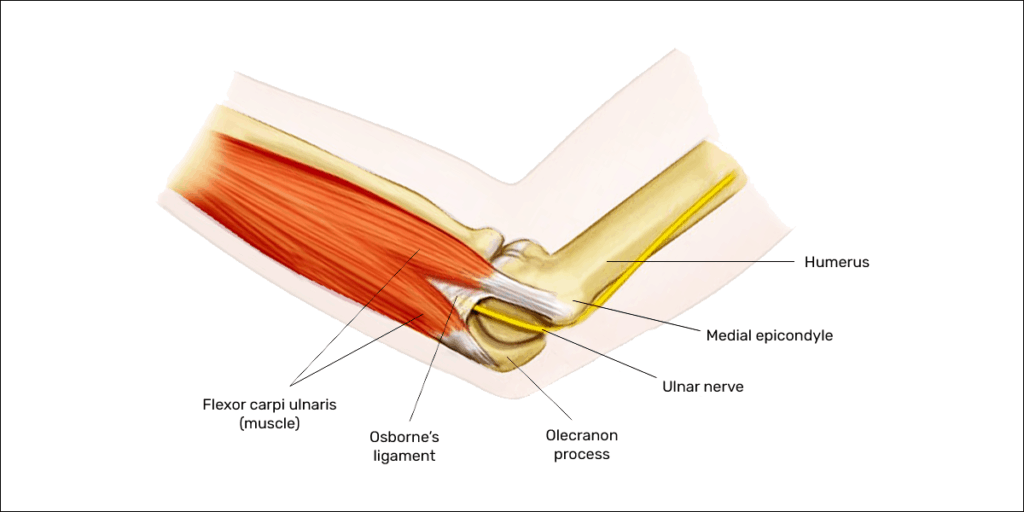
The only structure to pass through this passageway is your ulnar nerve. The boundaries of the cubital tunnel are:
- Floor: elbow joint capsule and medial collateral ligament (two types of fascia)
- Medial: medial epicondyle of the humerus (upper arm bone)
- Lateral: olecranon process of the ulna (one of two forearm bones)
- Roof: Osborne’s ligament (a band of fascia connecting the two bellies of the flexor carpi ulnaris muscle)
Ulnar nerve
The ulnar nerve innervates many muscles below your elbow:
- Muscles in the forearm
- Flexor carpi ulnaris: flexion (bending towards your palm) and ulnar deviation (bending towards your pinky) of your wrist
- Flexor digitorum profundus (medial half): flexion (closing) of your pinky and ring finger, including the finger tips
- Muscles in the hand
- Opponens digiti minimi: opposition of the pinky finger to the thumb
- Abductor digiti minimi: abduction (separation) of your pinky finger away from the ring finger
- Flexor digiti minimi brevis: flexion of your pinky finger
- The third and fourth lumbrical muscles: flexion of the knuckles of your ring and pinky finger
- Dorsal interossei: abduction (separation) of your fingers
- Palmar interossei: adduction (bringing back together) of your fingers
- Adductor pollicis: adduction of your thumb (bringing the thumb back to your palm)
- Flexor pollicis brevis (deep head): flexion of your thumb
- Palmaris brevis: squeezes the base of your hand
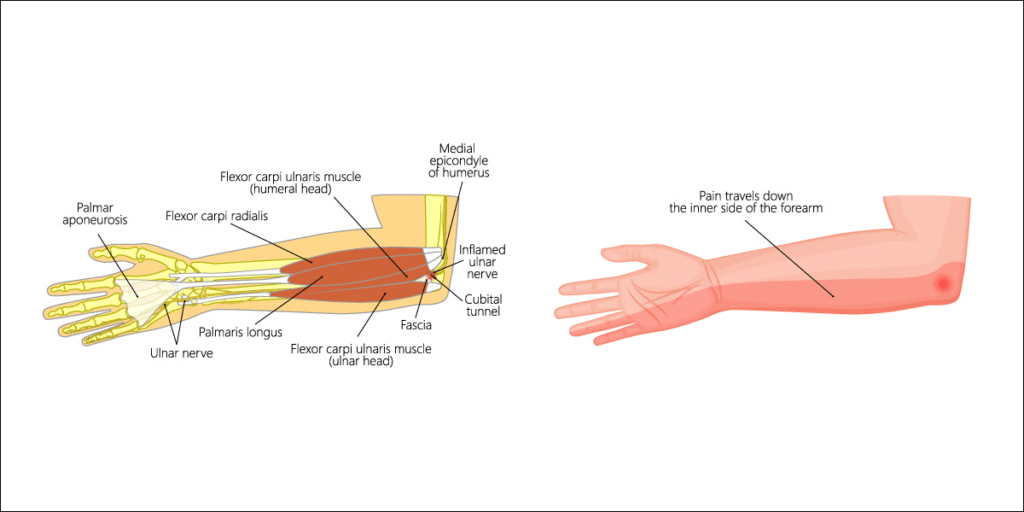
The ulnar nerve is also responsible for touch sensation for a large portion of your hand. The cutaneous innervation (touch sensation, see image below) includes:
- Your pinky finger and medial half of your ring finger
- The pinky side of your hand, both front and back
The ulnar nerve DOES NOT provide touch sensation to your thumb, index, middle finger, or the corresponding portion of your hand!
Pathophysiology
Cubital tunnel syndrome occurs when there is compression or irritation of the ulnar nerve within the cubital tunnel. The compression or irritation may be caused by:
- Inflammation
- Injury: elbow injuries (sprains, strains, trauma, etc.) may cause inflammation which may narrow the space within the cubital tunnel
- Movement imbalance: repetitive, inappropriate movement may lead to chronic muscle tightness which can compress the cubital tunnel and the ulnar nerve
- Specifically, medial epicondylosis, an ailment related to movement imbalance, may lead to or exacerbate cubital tunnel syndrome
- Tension on the ulnar nerve
- Prolonged, static position: if the elbow is flexed (bent) completely for a long period of time, the ulnar nerve is pulled taut and may begin to cause symptoms
- Direct compression of the ulnar nerve
- Leaning on the elbows: resting the inner portion of the elbows on another surface, such as your thighs or armrests, may place direct pressure over the cubital tunnel and the ulnar nerve
- Striking your elbow: commonly identified as the “funny bone,” striking the back of your elbow often causes transient symptoms of ulnar nerve insult; however, this would not be a true cubital tunnel syndrome
Signs and symptoms
If you’re affected by cubital tunnel syndrome, you may experience one or more of the following symptoms:
- Numbness and tingling
- The first sign is usually a change in sensation of your pinky, ring finger, and the pinky side of your hand and forearm
- These changes in sensation most often present as pins and needles, tingling, or numbness
- Weakness
- The weakness will be most prevalent in flexion of your pinky and ring finger
Note: cubital tunnel syndrome does not cause any of the above listed symptoms in the thumb, index, middle finger, or corresponding portion of your hand. Those symptoms are more consistent with carpal tunnel syndrome.

Other common findings may include:
- More pronounced symptoms with flexion of your elbow (e.g., talking on the phone) or leaning of your elbows or forearms on any surface
- Relief or improvement of symptoms with straightening of your elbow
Note: paleness or blue color and/or cool or cold sensation along with tingling and numbness may be indicative of blood flow occlusion. This may be a more serious condition, and you should consult your doctor or visit the emergency room if you are concerned about these symptoms.
Common mechanism(s) of injury
Cubital tunnel syndrome is more common for console gamers due to the handling of a controller and resting of the elbows and forearms. Common risks for console gamers include:
- Direct compression
- Leaning on your forearms or elbows may cause direct compression of the ulnar nerve; resting the elbows or forearms on your thighs or armrests are common causes
- Prolonged elbow flexion
- Bending your elbows puts tension on the ulnar nerve; prolonged flexion of your elbows will eventually lead to symptoms
- Movement imbalance and chronic muscle tightness
- Movement imbalance of your flexor muscles from movements such as pressing buttons and triggers may eventually lead to muscle tightness in your forearms (see medial epicondylosis).

Preventing cubital tunnel syndrome
For all common gaming injuries, we’ve created a comprehensive injury prevention program. Performing this exercise routine may help reduce your risk for cubital tunnel syndrome.
The most common mechanisms of injury for cubital tunnel syndrome are direct compression of the ulnar nerve and poor and/or prolonged static position.
Elbow position: it is important to keep your elbows relatively neutral (see our posture page for more information):
- For console gamers, allow your elbows to relax so you’re not creating tension in the ulnar nerve
- For both console and PC gamers, be sure you’re not resting the inside of your elbows on your armrests or thighs
- If you’re resting your elbows, rest on the bony portion on the back of your elbow
- For both PC and console gamers, between games/matches:
- Flex and extend your elbows a few times
- Turn your palms upward and downward a few times
As with all injuries and ailments of the upper extremities (arms):
- Take breaks to avoid overuse
- Be sure to warm-up your hands and wrists prior to gaming
- Perform the proper stretches when you’re done with your sessions
Rehabilitation
Correcting ergonomics is often enough to relieve symptoms of cubital tunnel syndrome. Avoiding compression and tension will usually begin the healing process.
In practice, the following treatments are effective for improving the rate of recovery for cubital tunnel syndrome:
- Massage of the wrist and finger flexor muscles at the medial forearm
- Contrast therapy: heat therapy followed by cold therapy
- Therapeutic exercises
- Functional Range Conditioning (FRC®): wrist PAILs/RAILs
- Wrist and hand mobility exercises (FRC®: wrist CARs)
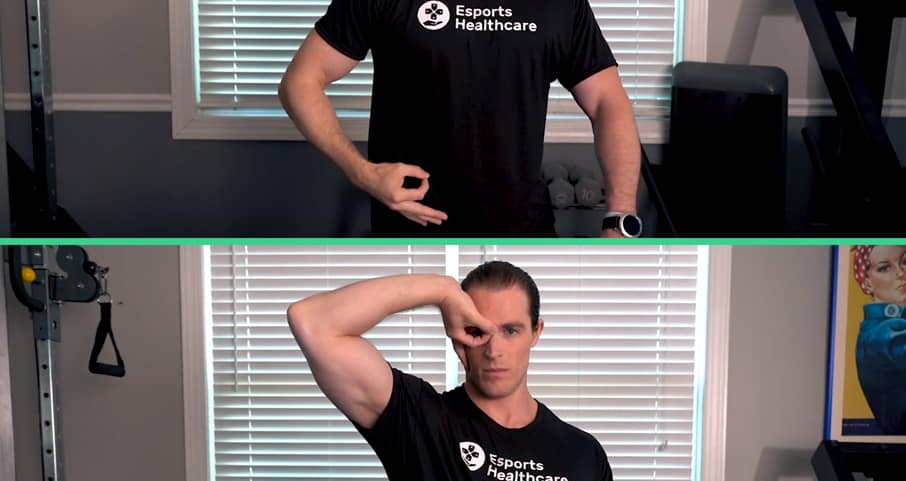
- Ulnar nerve glide (see our Injury Prevention Program for more information)
- Education in proper ergonomics
Following resolution, continuation of these protocols allows for prevention of this condition from reoccurring.